

Nipple Pain and Trauma - Prevention and Cure
 To understand what is happening when attachment and breastfeeding are painful and nipples become sore and damaged, you first need to understand precisely how a newborn baby takes a deep comfortable effective mouthful of breast. This process is clearly described and illustrated in Rebecca’s education materials.
To understand what is happening when attachment and breastfeeding are painful and nipples become sore and damaged, you first need to understand precisely how a newborn baby takes a deep comfortable effective mouthful of breast. This process is clearly described and illustrated in Rebecca’s education materials.
We need to begin with the old adage that you have to know the normal before you can identify the abnormal.
How a healthy hungry newborn baby takes a deep latch.
To attach deeply at the breast a baby uses a forward reaching lower jaw and tongue combined with suction in the mouth to draw in enough breast to fill the baby’s mouth. The nipple ends up at the back of baby's mouth and breast behind the nipple fills the baby's oral cavity.
As the baby takes the breast (beginning from below the nipple first) suction in the mouth creates a vacuum which causes the breast to be ‘latched’ against all the surfaces of baby’s mouth. The extended tongue cradles the underside of the breast on the floor of the mouth, the top surface of the breast is vacuumed against the hard palate, while the fat pads in the newborns cheeks are sucked in to fill the gaps at the side of the mouth. The breast remains latched in this position until baby releases the vacuum at the end of the feed.
Tip: The most effective and gentle way to take a baby off the breast is to carefully insert a finger into the corner of baby’s mouth and slide it along the side of the gums, this lifts the fat pad away from the gums and breaks the vacuum.
When attachment is deep and comfortable “Roughly a third of the mouthful is nipple, the rest needs to be breast. Babies breastfeed – they don’t nipple feed.” (Pamphlet – Key to Successful Breastfeeding © Rebecca Glover 1997 – 2012)

With the breast in this position the nipple comes to rest at the back of baby’s mouth, within 5mm of the junction of the hard and soft palate, (Jacobs L.A. 2007) a safe place where, with normal feeding anatomy, it will not be pinched, abraided or damaged. (Note - There is a wide range of normal anatomical variability, but there are anatomical variations that can interfer with latch)
The most common causes of nipple pain and trauma
The primary cause of nipple pain and trauma is shallow attachment. Which occurs when something interferes with a baby’s ability to take a deep enough mouthful of breast.
The contributing causes of a shallow latch include:
- Positioning and attachment techniques that interfere with a baby’s innate latching behaviours.
- Anatomical variations such as:
An excessively receding jaw – often associated with a short tongue and tongue tie
Ankyloglossia - Tongue tie
High or narrow hard palate
There are some causes of nipple pain such as Candida or other infections and Vasospasm of the nipple that are often but not always related to a shallow latch that I will not cover in this article.
When breastfeeding is painful it appears that a baby may be trying to compensate for or correct the shallow attachment, with increased sucking vacuums (McClellan H.L. 2008) or behaviours that causes pressure or friction on the nipple such as trying to hold the breast in the mouth with their lips or gums.
Unless a mother can find effective help at this stage the result is often an extremely painful physical and emotional downward spiral of events that end in a mother having no alternative than to give up breastfeeding.
 Preventing Nipple Pain and Trauma
Preventing Nipple Pain and Trauma
The positioning and attachment techniques described in Rebecca’s education materials and on this website have been shown to significantly reduce the incidence of attachment difficulties, sore and damaged nipples, and to increase breastfeeding duration rates at 6 weeks postpartum. (Duffy E 1997)
The Effect of a Prenatal Teaching Intervention on Postpartum Nipple Pain and Trauma. Duffy E.P. 1997
The study used an experimental design with random allocation of primigravida mothers to an experimental or control group. The researcher was observer blind to group allocation until completion of all observations on the 4th day.
Methodology:
- 70 primigravida women of >36 weeks gestation were recruited from a hospital A/N clinic
- 78% of participants attended the all four hospital A/N classes (In the experimental group only 3 did not attend)
- A questionnaire was developed to collect background information
- There were no significant differences for any demographic or obstetric variables - Significantly a low income group
- The experimental group in this study (n 35) had a one hour practical and interactive session with Rebecca, in groups of 6-8. Together they used lifelike soft bodied dolls (each mother had one), Rebecca’s Pamphlet – The Key to Successful Breastfeeding (1991 edition) (each mother went home with a pamphlet) and the Attachment teaching chart to demonstrate, describe and role play newborn latching behaviours.
- After birth the women were interviewed by the researcher daily for the 1st 4 days postpartum
- At 6 weeks they had a follow up phone interview
- The study proposed 4 hypotheses - That the women in the experimental group would experience:
- 1: Significantly better positioning & attachment
- 2: Significantly less nipple pain
- 3: Significantly less nipple trauma
- 4: Significantly Increased breastfeeding rates at 6 weeks

Content of the Interactive Session:
In the session Rebecca explained to the women how a baby needed to take the breast and nipple to attach deeply and prevent painful attachment, painful feeding and damage to the mothers nipples.
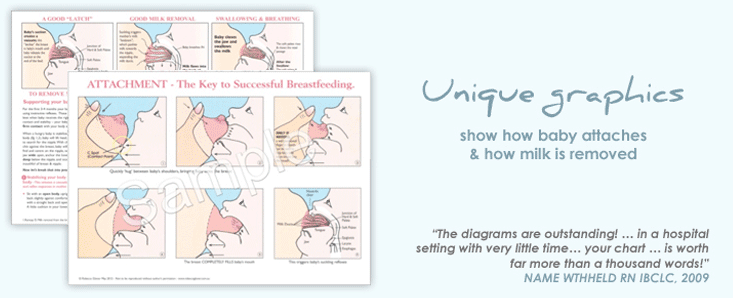
Using her unique graphics to describe:
A Good Latch – the position of the breast and nipple in the mouth and why it was important
How and why a baby needs to take more of the breast below the nipple
How and why a baby needs to approach the breast chin first, head tilted back – the instinctive position and comfortable drinking position for baby.
How a baby takes a deep asymmetrical latch.
How a well attached baby effectively removes milk from the breast.
 Using the dolls, Rebecca modeled and the mothers copied the simple steps of the positioning and attachment process:
Using the dolls, Rebecca modeled and the mothers copied the simple steps of the positioning and attachment process:
How a hungry healthy baby is built to respond, reaching up for the breast and adopting the breastfeeding baby’s instinctive feeding position.
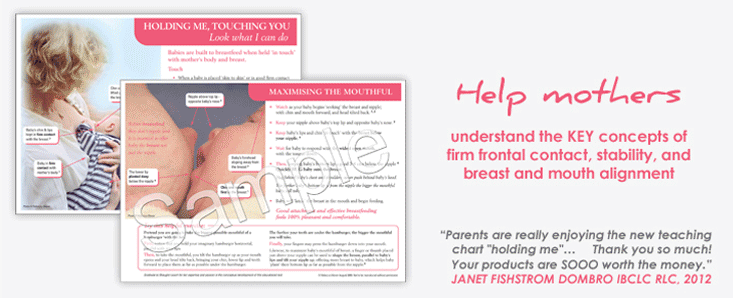
How to hold and where to position and stabilize their baby dolls against their body and breast
How to tilt the nipple up to offer baby more breast below the nipple to help their baby take a deep comfortable mouthful of breast.
How to ‘hug’ baby behind the shoulder blades, when baby had a wide opened mouth with the bottom lip 3-4 cms below the nipple
At the end of the session Rebecca had worked individually with each women to ensure they had understood and experienced the behaviours that would help their baby attach well.
Results:
Instrument - LATCH assessment instrument (Jensen, Wallace & Kelsay, 1994 J Obs Gyn & Neonatal Nrs 23 (1) 27-32
Higher scores equal better attachment
Results: In both groups the scores increased each day but the increase was only statistically significant in the experimental group.
Overall LATCH score: Experimental: M = 35.2, SD = 3.1 Control: M = 24.1, SD = 4.6
Hypothesis 2. Significantly less nipple pain - first 4 days postpartum
Instrument: Visual Analogue Scale (VAS) Clark P. Spear F. (1964)
No Pain _________ Pain as bad as it could possibly be.
Results:
Experimental Group: Experienced Less pain on each of the 4 days, with a high percentage experiencing no pain.
M = 3.7 SD = 4.1 Control: M = 23.5 SD = 9.2
Controls: Pain increased daily, worst on day 4
All experienced pain on days 2,3, & 4.
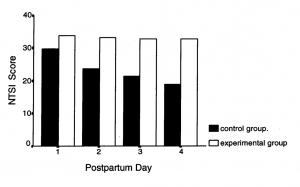
Hypothesis 3. Significantly less nipple trauma - first 4 days postpartum
Instrument: Nipple Trauma Severity Index (NTSI) - developed & tested for the research. The highest score = less trauma, the highest possible score was 136.
Results:
 Experimental Group:
Experimental Group:
Significantly less trauma - No further trauma from day 3
Exp: M = 132.85 SD = 5.5 Con: M = 94.20 SD = 16.3
Controls:
Scores increased each day, indicating increased nipple trauma each day
Hypothesis 4. Increased breastfeeding rates at 6 weeks
Follow-up telephone questionnaire at six weeks
Results:
Experimental Group: 32 were Fully Breastfeeding
Controls: 10 were Fully Breastfeeding
Qualitative Analysis - Comments from mothers and midwives
Following completetion of the questionnaire on day 4, many participants in the study added comments about their experiences which were later analysed.
Mothers: Experimental Group
“When they handed me my baby, I just knew what to do, I knew how to feed her. I didn’t know where I got the knowledge. Then I realised two days later that I had learned it at the class”
"The special teaching class gave me so much confidence. It was wonderful to have all that knowledge about something before you actually do it. I didn't worry then when the staff told me to do things differently. I just knew that the way Rebecca told us was the right way, as it made so much sense."
"I would recommend that teaching class to everyone who is going to breastfeed. It just made so much sense. You came away from it with so much knowledge. It was expecially good to be able to hold a doll for the demonstration of position and attachment, it helped me remember what to do when I started to breastfeed. I'm just glad I was in the group that went to the teaching class. But if I had not been in that group, I would never have known how beneficial it was."
“Every mother should have that teaching class before they start to breastfeed. I didn’t realise I knew so little … I thought it would all come naturally, all that bit about position and attachment, I never heard of it before, but now that I am doing it, it makes so much sense. You just know she is on the breast properly and that she is getting the milk”
Midwives Comments:
A noticeable increase in mothers’ knowledge about breastfeeding
Mothers more confident breastfeeding their baby
Staff needing to spend less time with the breastfeeding mothers
Mothers less anxious, even when they were having difficulties
Mothers: Control Group
“I just don’t seem to be able to breastfeed. Every time I put him on the breast he screams, he’s screaming all the time. My nipples are so painful and they are cracked.”
“When I was having problems breastfeeding in those first few days, I lost all confidence in myself as a mother.”
"I just lost all confidence in myself when I wasn't able to breastfeed, everthing seemed to go wrong then... I cried a lot. It was better when I gave her the bottle."
When a baby is struggling to attach deeply, mothers can quickly learn, via interactive coaching (participatory modeling) how to work with and support their baby's innate reflex latching behaviours to help them achieve a deep comfortable and effective latch.
© Rebecca Glover Nov 2012
