

L.A.T.CH.O. - Learned Attachment Techniques CHanges Outcomes
Breastfeeding Natural? YES! – Comes Naturally?
For a mother breastfeeding has a 'learned' component, but for her newborn baby, breastfeeding is entirely instinctive.
Natures way for mothers to learn, is by subconsciously observing other mothers successfully holding, positioning, and attaching their babies.
As breastfeeding is a basic survival behavior it is not surprising that recent evidence suggests that mothers also have some instinctive breastfeeding behaviours - given the right environment.15.
This does not mean that mothers don’t learn subconsciously from their cultural experiences, because that is precisely how the human brain works. The more often we see, perform or even think about a particular behavior, stronger and more lasting neural pathways develop in our brain. "Neurons that fire together wire together" 4.
Today women rarely have the opportunity to observe successful newborn positioning and attaching behavior. This means a new mother may not understand how to work with her baby’s instinctive latching behaviors, unless someone models or explains them for her.
Health professionals and lay counselors who work with new mothers and babies play an important role when they help a new mother to understand and support her baby’s instinctive breastfeeding reflexes.10.
Follow Me Mum, I do this instinctively!
The first 3-4months of life are a unique period for the human infant. When feeding behaviour is entirely instinctive and reflex and the infants anatomy is uniquely designed to match the behaviours.1.2.5.6.7. These reflex behaviours are dependent on; appropriate sensory input, (physical contact) adequate stability (positional) and the maturity and normal function of the baby’s physical structures. 7.
Sensory Input – Touch – Physical Contact: When a baby is placed ‘skin to skin’ or in firm full frontal contact with its mother body and breast this releases a cascade of hormonal responses in both mother and baby. Which include becoming calm and focused on each other and the feeding process. This firm physical contact also triggers the baby’s instinctive reflex attaching behaviours. 13.14.
The “Instinctive Position” - a distinctive instinctive feeding posture 4.

When newborn to 3-4 month old infants are provided with the appropriate sensory input on mothers’ body and breast, they instinctively begin 'seeking' the breast. Lifting the chin, they reach up to find the breast and nipple - chin and mouth forward, head tilted backwards. This “Instinctive Position” moves a baby's external and internal anatomy into the optimal position for strong controlled reflex movements. 1.2.3.5.7.8.
A deep latch is difficult or even physically impossible with baby’s chin down; try swallowing with your chin dropped towards your chest, uncomfortable isn’t!
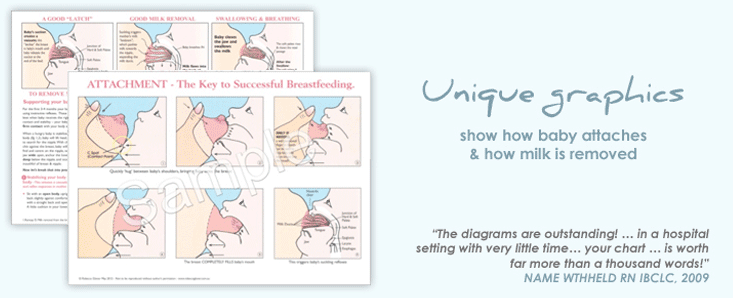
To make Good Attachment physically possible babies need to approach the breast in the “instinctive position” to allow a baby’s mouth to open wide with the tongue extended, ready for baby to “scoop” up a good amount of breast with the tongue and lower jaw. The nipple rolls back, close to the junction of the hard & soft palate, and the breast fills baby’s mouth with the tongue & lower jaw positioned deep under the breast tissue below the nipple. 5.6. (see Rebecca’s unique graphics)

This essential mouthful provides the appropriate sensory input (everything touching in baby’s mouth) for baby to begin breastfeeding comfortably and effectively.
Baby removes milk from the breast by a combination of mothers milk ejection reflex pushing milk into baby’s mouth, as increased suction at the back of baby’s mouth pulls milk out of the breast when baby lowers the tongue and jaw during suckling. 12. (shown in Rebecca's unique graphics in her Pamphlet, Attachment Teaching Chart, Attachment Poster)
The Magic of Positional Stability7.8.
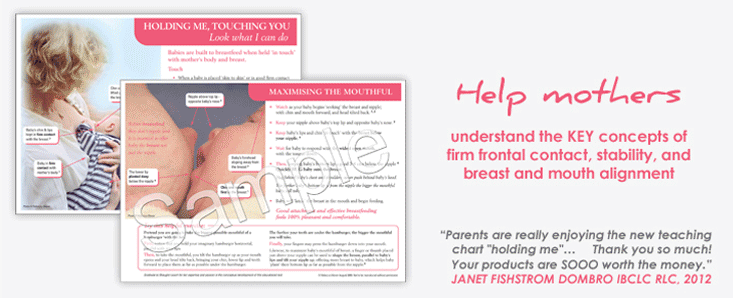
To attach well and breastfeed effectively a newborn infant is totally reliant on external support - positional stability.
Without a stable base function and movement is less controlled or even impossible. Therefore, for the infant to control and perform the complex oro-motor movements required for attachment and breastfeeding they must be provided with the appropriate stability - firm frontal contact on mothers body. 7.
Head, neck and Oral Stability is also dependent on shoulder girdle stability, which is in turn, dependant on trunk and pelvic stability.7.8.
 To support the reflex latching behaviours young infants require:
To support the reflex latching behaviours young infants require:
Midline Stability – baby’s body centrally straight from head to toe
This supports the symmetrical movement of the muscles on both sides of baby’s body.
Shoulder Girdle Stability – Baby receives shoulder girdle stability via gravity in laid-back breastfeeding positions or when mother holds her baby on or between the shoulder blades. This stabilises the neck, head, jaw, tongue, pharynx & larynx to enable controlled and effective seeking, attaching and suckling movements.
Trunk and Pelvic Stability – shoulders and hips turned towards and supported against the mothers’ body.
Stabilized on mothers body a hungry baby will lift his head, chin and mouth to search for the nipple. Stimulated by the touch of his face (cheeks-lips-chin) on the breast, baby instinctively moves to, and centres his mouth on, the nipple, his lower jaw swings wide open to anchor (bottom lip and chin) on the breast before scooping breast and nipple into his mouth.
Rebecca’s education materials demonstrate how this process happens in practice, whether a mother simply wishes to speed up the process by bringing her baby directly to the breast, or needs to step in and help her baby who cannot attach on his/her own.
Watching a mother working WITH her baby’s innate latching behaviours, is pure magic to behold; especially when major attachment difficulties are resolved through such simple and empowering methods.
References
- Widström A-M et al. Gastric suction in healthy newborn infants. Effects on circulation & developing feeding behaviour. Acta Paediatr Scand 1987;76:566-72
- Righard L. Alade M.O. Effect of delivery room routines on success of first breastfeed. Lancet 1990;336:1105-07
- Bergman N.J. Humans & Kangaroos – A Biological Perspective. Conference Syllabus. ILCA 2003 Sydney. www.kangaroomothercare.com
- Doidge, N. (2010). The brain that changes itself. New York, NY: Penguin Group.
- Woolridge M.W. The ‘Anatomy’ of Infant Sucking. Midwifery 1986;2:164-171
- Woolridge M.W. Aetiology of Sore Nipples. Midwifery 1986;2:172-176
- Wolf L.S. Glass R.P. Feeding and Swallowing Disorders in Infancy: Assessment and Management. 1992 Therapy Skills Builders
- Evans-Morris S. Klein M.D. Pre-Feeding Skills. 1987 Therapy Skills Builders
- Glover R. Hold Tight – Feed Right. The Promise of Positional Stability. Conference Syllabus. ILCA 2003 Sydney Australia
- Glover R. Lessons from Innate Feeding Abilites Transforms Breastfeeding Outcomes. Conference Sylabus. ILCA 2004 Scotsdale Arizona USA.
- Glover, R., & Wiessinger, D. (2012). They Can Do It, You Can Help: Building Breastfeeding Skill and Confidence in Mother and Helper In C. Watson Genna (Ed.), Supporting Sucking Skills in Breastfeeding Infants (pp. 105-148). Woodhaven, New York: Jones & Bartlett
- Ramsay D.T. Hartmann P.E. Milk removal from the breast. Breastfeeding Review 2005: 13(1): 5-7
- Uvnas Moberg, K., and M. Eriksson. Breastfeeding: Physiological, endocrine and behavioural adaptations caused by oxytocin and local neurogenic activity in the nipple and the mammary gland. Acta Paediatrica Scandinavica 1996:85, 525-530
- Uvnas Moberg, K. (2003) The Oxytocin Factor (pp 95-99) Decapo Press, Perseus Books Group
- Colson, S. D., Meek, J. H., & Hawdon, J. M. (2008). Optimal positions for the release of primitive neonatal reflexes stimulating breastfeeding. Early Human Development, 84(7): 441-449.
© Rebecca Glover June 2003 (Updated Jan 2012)
May be copied for individual educational purposes only. All other reproduction prohibited unless written permission is obtained from the author.
